
Abstract
We conducted a systematic review and meta-analysis to evaluate the efficacy and safety of TZDs in treatment of diabetes mellitus patients with renal impairment. We searched PubMed, EMBASE and Cochrane Central Register of Controlled Trials. Randomized controlled trials (RCTs), cohort studies, and case-control studies that investigated the effects of TZDs in patients with diabetes and renal impairment were eligible. Outcomes included glycosylated hemoglobin, fasting plasma glucose, serum lipids, and patient-important outcomes (i.e. hypoglycemia, weight, edema, cardiovascular events and mortality). 19 RCTs and 3 cohort studies involving 21,803 patients with diabetes and renal impairment were included. Meta-analysis of RCTs showed that TZDs could significantly reduce HbA1c (MD −0.64, 95%CI −0.93 to −0.35), FPG (MD −26.27, 95%CI −44.90 to −7.64) and increase HDL levels (MD 3.70, 95%CI 1.10, 6.29). TZDs could increase weight (MD 3.23, 95% CI 2.29 to 4.16) and risk of edema (RR 2.96, 95% CI 1.22 to 7.20). Their effects on risk of hypoglycemia (RR 1.46, 95% CI 0.65 to 3.29), heart failure (RR 0.64, 95% CI 0.15 to 2.66), angina (RR 1.45, 95% CI 0.23 to 8.95) and all-cause mortality (RR 0.40, 95% CI 0.08 to 2.01) are uncertain. Results from cohort studies were similar to RCTs.
Similar content being viewed by others

Introduction
The prevalence of diabetes mellitus continues to rise worldwide1. Chronic kidney disease, a common complication in diabetes patients, has recently become the leading cause of end-stage renal disease (ESRD) requiring dialysis in most countries2.
Treatment options for diabetic patients with chronic kidney disease is limited, especially in patients with ESRD. With their deteriorated renal function, many oral hypoglycemic drugs (e.g. metformin) are not recommended for patients with severe chronic kidney disease3. The thiazolidinediones (TZDs) (rosiglitazone and pioglitazone) are activated receptor gamma (PPAR-γ) antidiabetic agents, and are mainly metabolized by liver. They do not require dose adjustment in patients with renal impairment4, 5, and may have renal protective effects. A meta-analysis indicated that treatment with TZDs significantly decreased urinary albumin and protein excretion in patients with diabetes6. In addition to renal benefits, pioglitazone has been shown to improve a number of intermediate markers of cardiovascular diseases, such as blood pressure and serum lipids7.
However, cardiovascular safety of TZDs in patients with diabetes mellitus patients has become a matter of major controversy, especially for rosiglitazone. Several meta-analyses showed that the risk of myocardial infarction (MI) and heart failure was significantly increased by rosiglitazone8, 9. In 2007, US Food and Drug Administration (FDA) restricted treatment of rosiglitazone only in new patients who are unable to achieve glucose control with other drugs or unable to take pioglitazone, and current users who are benefiting from this drug and choose to continue using it10. The Rosiglitazone Evaluated for Cardiac Outcomes and Regulation of glycaemia in Diabetes (RECORD) study, however, did not rule out an elevated risk of myocardial infarction amongst participants treated with rosiglitazone11. The Veterans Affairs Diabetes Trial (VADT) even found that use of rosiglitazone was associated with decreased risk of cardiovascular composite outcome and cardiovascular death12. Recently FDA repealed restriction of rosiglitazone. Though accumulating studies focused on cardiovascular safety of TZDs treatment, most of these studies excluded patients with obvious renal impairment. The safety of TZDs in treatment of diabetes patients with renal impairment has still been uncertain. Considering high prevalence of cardiovascular events in patients with renal impairment, whether TZDs increase the risk of heart failure, myocardial infraction and mortality has been a major concern of clinician.
Most of reported studies of TZDs treating in diabetes patient with renal impairment were small sample sizes (especially in randomized control trials) and had conflicting findings on cardiovascular outcomes13,14,15,16,17. A cohort study found that TZDs use was associated with better survival in hemodialysis patients with type 2 diabetes14, but another cohort study found that diabetes patients prescribed rosiglitazone had significantly higher all-cause mortality and cardiovascular mortality15. Except for mortality, whether treatment of TZDs in diabetes patients with renal impairment increase the risk of heart failure was inconsistent16, 17. Though guideline approved treatment of TZDs in patients with chronic renal failure2, 18, but these recommends mainly based on pharmacokinetics not clinical researches.
Consequently, we conducted this systematic review and meta-analysis to investigate the efficacy and safety of TZDs in treatment of patients with diabetes mellitus and renal impairment.
Results
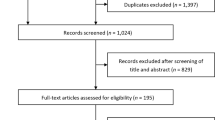
We identified a total 1,936 potentially relevant reports in the initial retrieval. Finally, 22 studies were included in data analysis, including 19 RCTs (n = 1,818) and 3 cohort studies (n = 19,985) (Fig. 1).

Flow chart of article selection.
Study characteristics
Table 1 summarized the characteristics of the 22 included studies. The 19 RCTs involved a total of 1,818 participants, with mean age ranging from 43.4 to 71.1 years, mean baseline HbA1c 6.9 to 9.2%, mean fasting plasma glucose 135.7 to 205.2 mg/dl, and mean duration of diabetes 5.5 to 17.5 years. Of the 19 RCTs, one (5.3%) enrolled patients undergo renal transplantation, five (26.3%) enrolled dialysis patients, and thirteen (68.4%) trials included patients with mild to moderate renal impairment. Fourteen (73.7%) trials used pioglitazone as intervention, four (21.1%) used rosiglitazone, one (5.3%) used both pioglitazone and rosiglitazone.
Of the three cohort studies, one was prospective and two were retrospective studies. These cohort studies included a total of 19,985 participants; mean age ranged from 63.5 to 66.1 years and mean follow-up 24 week to 270 days. All these cohort studies enrolled ESRD patients.
Risk of bias assessment
All the 19 RCTs were at moderate to high risk of bias16, 17, 19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35 (Supplementary Table 1). Of the three cohort studies, one15 was at low risk of bias, one moderate risk14 and another36 high risk. (Supplementary Table 2).
Publication bias assessment
Publication bias was investigated using the funnel plot and Egger’s tests. No evidence of publication bias was found for the outcomes of FPG, HbA1c, TC, TG, and HDL. Owing to the limited numbers of the included studies or low events rate, publication bias investigation was not performed for other outcomes.
Efficacy of TZDs
HbA1c
Fifteen RCTs reported change of HbA1c from baseline. Compared with all controls, HbA1c in TZDs group significantly decreased, with substantial statistical heterogeneity (MD −0.64, 95% CI −0.93 to −0.35, I2 = 69%) (Fig. 2). Subgroup analysis showed that, compared with placebo or no additional drugs, levels of HbA1c in TZDs groups were significantly lower (MD −0.90, 95% CI −1.24 to −0.56, I2 = 73%), while no significance between groups was observed when compared with active drugs (MD −0.16, 95% CI −0.50 to 0.18, I2 = 0%; test for subgroup differences: P = 0.003) (Supplementary Table 3).

Change in HbA1c among patients with diabetes mellitus and renal impairment receiving TZDs versus control from RCTs.
Fasting plasma glucose
Changes in FPG from baseline were reported in 10 RCTs. Compared with controls, treatment of TZDs was associated with a significant decrease in FPG levels, with considerable statistical heterogeneity (MD −26.27, 95% CI −44.90 to −7.64, I2 = 89%) (Fig. 3). Subgroup analysis showed that, when compared with placebo or no additional drugs, TZDs significantly decreased FPG levels (MD −32.26, 95% CI −53.13 to −11.39, I2 = 90%); comparison with active drugs as controls illustrated a lack of significant effect (MD 3.94, 95%CI −12.96 to 20.84, I2 = 0%; test for subgroup differences: P = 0.008) (Supplementary Table 3).

Change in FPG among patients with diabetes mellitus and renal impairment receiving TZDs versus control from RCTs.
Serum lipids and lipoproteins
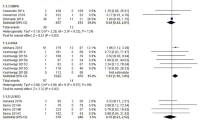
A total of 11 trials reported changes in triacylglycerol (TG). Compared with controls, TG in TZDs group had no significant decrease (MD −17.18, 95% CI −37.25 to 2.90, I2 = 61%) (Fig. 4A). Subgroup analysis showed that, compared with controls, levels of TG in pioglitazone group were significantly lower (MD −26.38, 95% CI −40.56 to −12.19, I2 = 25%); no significance was observed between rosiglitazone group and controls. (MD 31.81, 95% CI −24.73 to 88.35, I2 = 61%; test for subgroup differences: P = 0.05) (Supplementary Table 3).

Changes in serum lipids and lipoproteins among patients with diabetes mellitus and renal impairment receiving TZDs versus control from RCTs. (A) Change in triacylglycerol (TG), (B) Change in total cholesterol (TC), (C) Change in low-density lipoprotein (LDL), (D) Change in high-density lipoprotein (HDL).
Twelve trials reported changes in total cholesterol (TC), no significant differences between groups were observed in the analysis of TC (MD −0.02, 95% CI −8.04 to 8.00, I2 = 31%) (Fig. 4B). Subgroup analysis showed that, compared with controls, treatment of pioglitazone significantly decreased TC levels (MD −7.00, 95% CI −13.77 to −0.23, I2 = 0%), but treatment rosiglitazone significantly increased TC levels (MD 13.51, 95% CI 0.48 to 26.54, I2 = 0%; test for subgroup differences: P = 0.006) (Supplementary Table 3).
Five trials reported changes in low-density lipoprotein (LDL). There were no significant changes in LDL levels between TZDs group and controls (MD 4.49, 95% CI −6.44 to 15.43, I2 = 53%) (Fig. 4C). Subgroup analysis showed that, compared with controls, LDL levels had no significant decrease both in pioglitazone group (MD 8.30, 95% CI −12.82 to 29.41, I2 = 73%) and rosiglitazone group (MD 4.66, 95% CI −6.61 to 15.94, I2 = 0%; test for subgroup differences: P = 0.77) (Supplementary Table 3).
Ten trials reported changes in high-density lipoprotein (HDL). HDL in TZDs group was significant increase, and the heterogeneity was moderate (MD 3.70, 95% CI 1.10 to 6.29, I2 = 42%) (Fig. 4D). Subgroup analysis by type of TZDs showed that treatment of pioglitazone (MD 4.84, 95% CI 2.50 to 7.18, I2 = 22%), but not rosiglitazone (MD −1.92, 95% CI −6.66 to 2.82, I2 = 0%; test for subgroup differences: P = 0.01), significantly elevated HDL levels (Supplementary Table 3).
Safety of TZDs
Hypoglycemia
Six trials involving 1,178 participants reported hypoglycemia, of which two trials17, 23 compared TZDs versus active drugs (sufonylureas, DPP-4), and four trials16, 21, 25, 27 compared TZDs versus placebo/no additional drugs. One trial23 used both rosiglitazone and pioglitazone as intervention, four trials16, 17, 25, 27 used pioglitazone and one trial21 used rosiglitazone as intervention. Meta-analysis suggested that, compared with controls, there was no significant differences between groups in the risk of hypoglycemia and the heterogeneity was low (RR 1.46, 95% CI 0.65 to 3.29, I2 = 0%) (Supplementary Fig. 1).
One cohort study36 involving 12,350 participants reported hypoglycemia. There was no significant difference in the risk of hypoglycemia between TZDs and control (RR 0.99, 95% CI 0.65 to 1.52).
Weight change
Five trials (n = 241) reported changes in weight, of which four trials enrolled patients with ESRD and treated patients with pioglitazone. All trials used placebo/no additional drugs as controls. Compared with control group, treatment of TZDs significantly increased body weight (MD 3.23, 95% CI 2.29 to 4.16, I2 = 0%) (Fig. 5). Of these five trails, two trials reported changes in dry weight. Considering there may be some differences between dry weight and total weight, we also did meta-analysis respectively. The results showed that total weight (MD 2.82, 95% CI 1.17 to 4.47, I2 = 38%), but not dry weight (MD 0.95, 95% CI −11.57 to 13.46, I2 = 0%) significantly increased in TZDs group. No cohort study reported weight changes.

Change in weight among patients with diabetes mellitus and renal impairment receiving TZDs versus control from RCTs.
Edema
Seven trials reported edema or worsening edema, of which three trials17, 23, 28 compared TZDs versus active drugs, five trials17, 21, 23, 24, 28 enrolled patients with non-ESRD, and the other two trials16, 20 included patients with ESRD. One trial23 compared TZDs (both rosiglitazone and pioglitazone) versus control, four trials16, 17, 20, 28 compared pioglitazone versus control and the other two trials21, 24 compared rosiglitazone versus control. Meta-analysis of seven RCTs showed that the risk of edema significantly increased in TZDs group compared with control (RR 2.96, 95% CI 1.22 to 7.20, I2 = 0%) (Fig. 6). We also did subgroup analyses by type of renal impairment, type of TZDs and type of control, but the subgroup differences had no statistical significance (Supplementary Table 3). No cohort study reported edema.

Risk of edema in patients with diabetes mellitus and renal impairment for the TZDs versus control groups from RCTs.
Cardiovascular events
Of the five trials (n = 233) reporting heart failure, one17 compared TZD versus active drugs (sulfonylureas), and the remaining four16, 26, 27, 33 compared TZDs versus placebo/no additional drugs. One trial33 used rosiglitazone as intervention and the other three trials used pioglitazone as intervention. Meta-analysis showed that TZDs-treatment did not increase the risk of heart failure (RR 0.64, 95% CI 0.15 to 2.66, I2 = 0%) (Table 2).
Three trials reported three angina events occurring in 168 patients. All these trials used pioglitazone as intervention. The pooling of those trials showed no statistically significant difference in the risk of angina between pioglitazone treatment and control (RR 1.45, 95% CI 0.23 to 8.95; I2 = 0%) (Table 2). Two trials16, 33 reported myocardial infarction, but no event occurred in each group. No study reported the data of stroke.
One trial34 (RR 0.33, 95% CI 0.01 to 7.82) and one cohort study15 (RR 1.23, 95% CI 0.87 to 1.75) reported cardiovascular mortality, both results showed that TZDs treatment may not increase the risk of cardiovascular mortality (Table 2).
All-Cause Mortality
Five trials involving 878 participants reported all-cause mortality, of which three trials17, 23, 28 compared TZDs versus active drugs (sufonylureas, DPP-4, metformin), two trials33, 34 compared TZDs versus placebo/no additional drugs. Meta-analysis showed that TZDs were not associated with increased risk of all-cause mortality (RR 0.40, 95% CI 0.08 to 2.01; I2 = 0%) (Table 2).
Meta-analysis of two cohort studies (n = 3,133) also showed that compared with control, TZDs did not increase the risk of all-cause mortality (RR 0.78, 95% CI 0.38 to 1.59; I2 = 85%) (Table 2).
We did sensitivity analyses using pooling methods and statistical models regarding heterogeneity, and the results (hypoglycemia, weight, risk of edema, HF, angina and all-cause mortality) were similar.
Discussion
In this study, we found that TZDs may achieve improved glucose control relative to placebo in patients with diabetes and impaired renal functions. We did not observe difference in the glucose control effects between TZDs and other anti-diabetes medications. However, the effects of the two individual agents of TZDs on serum lipids may differ – subgroup analyses suggested that pioglitazone could elevate HDL and reduce TG and TC, but not with rosiglitazone. Our study also found that TZDs did not increase the risk of hypoglycemia. Compared with controls, TZDs significantly increased the risk of weight gain and edema, but their effects on heart failure, angina, myocardial infraction, cardiovascular mortality and all-cause mortality were uncertain.
Several previous studies supported our findings. A meta-analysis37 found that metformin, TZDs and sulfonylureas had similar hypoglycemic effect, which explained our findings that the changes of HbA1c and FPG had no statistical significance when compared with active drugs. The PROspective pioglitazone Clinical Trial in Macrovascular Events (PROactive) found that compared with placebo, pioglitazone reduced HbA1c, TG levels and increased HDL levels38. A meta-analysis including 23 RCTs, which compared pioglitazone or rosiglitazone against placebo in patients with type 2 diabetes, found that pioglitazone elevated HDL levels and reduced TG levels, but rosiglitazone increased LDL and TC levels39. Although TZDs exerted effects in reducing glucose, our meta-analysis indicated that TZDs played no role in the risk of hypoglycemia. Possible explanation behind this mechanism is the fact that TZDs are mainly metabolized by the liver. Indeed, current clinical practice guidelines recommendations state that TZDs can be used in patients with renal failure as TZDs do not increase the risk of hypoglycemia2, 18.
Although the adverse effects of weight gain and edema in TZDs-treated patients were established11, 39,40,41, the effects of TZDs on cardiovascular events and mortality remain to be further explored. On one hand, our findings were consistent with a few published meta-analyses that found treatment with TZDs did not increase the risk of MI42, 43, cardiovascular mortality, or all-cause mortality44, 45. The PROactive trial even showed that treatment with pioglitazone significantly reduced the risk of all-cause mortality, non-fatal MI and stroke38. These benefits may also exist in patients without diabetes46. The mechanism for the observed phenomenon is unclear. Since endothelial dysfunction is a strong predictor for future cardiovascular events in patients with coronary artery disease47, 48, one possible explanation is that TZDs may have benefit on endothelial function. TZDs, PPAR γ agonists, could exhibit anti-inflammatory properties49, 50 and increase NO release from endothlial cells51, which may produce vasodilatation and attenuate vascular damage. Moreover, pioglitazone treatment could increase the number and function of endothelial progenitor cells (EPCs). Increased levels of EPCs, which enhance angiogenesis, promote vascular repair, and improve endothelial function52, could reduce the risk of cardiovascular mortality in patients with coronary artery disease48. In patients with type 2 diabetes, pioglitazone showed an effect on ameliorating endothelial dysfunction, which was independent of its metabolic action53, 54. Indeed, a randomized, placebo-controlled, double-blind trial found that, after six months treatment, pioglitazone group had a significantly better coronary endothelial function compare to control55, further supporting the hypothesis.
However, a couple of other meta-analyses suggested that treatment with TZDs might increase risk of MI8, 45. The reasons of these seemingly conflicts may be due to the inclusion of different TZDs in those studies. Previous studies showed that pioglitazone may reduce ischemic disease and all-cause mortality in patients with type 2 diabetes38, while rosiglitazone may increase cardiovascular events especially MI8, 9, 56. The underlying mechanisms for the apparent differences in cardiovascular risk and mortality have not been clearly understood, but one possible explanation is that the two class of TZDs may have different effect on lipids, as mentioned above. And lipid abnormalities may cause endothelial cell toxicity and subsequently induce endothelial dysfunction. Moreover, pioglitazone has shown some potential benefit in preventing progression of atherosclerosis57, but rosiglitazone failed to show any potential benefit in this regard58.
Our study has several strengths. Firstly, to the best of our knowledge, this is the first systematic review and meta-analysis on the topic of efficacy and safety of TZDs treatment in patients with different degree of renal impairment. A published meta-analysis illustrated that TZDs significantly decreased urinary albumin and protein excretion in patients with diabetes, but they enrolled patients with normoalbuminuria or proteinuria6. Secondly, we systematically identified and included both randomized and non-randomized studies. Compared to previous reviews, we assessed both efficacy and safety outcomes of TZD-treated patients using quantitative methods. However, our findings should be interpreted cautiously due to some limitations. First of all, the risk of bias of most eligible studies were moderate to high. Secondly, due to limited number of the included studies, some subgroup analyses were not carried out. We could not analysis whether different type of TZDs have different effects on hypoglycemia, CV events and mortality. Thirdly, lack of universal standard to definite outcomes may add heterogeneity to this analyses.
In summary, this meta-analysis suggests TZDs treatment in diabetes patients with renal impairment may improve glucose control and serum lipid, but may increase the risk of weight gain and edema. However, the effects of TZDs on cardiovascular events and all-cause mortality were uncertain, mainly because of the limited sample sizes and inadequate power. More carefully designed, conducted, adequately powered studies (both RCTs and observational studies) are warranted to examine the effect on the long-term patient important outcomes.
Methods
We followed the standards set by Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA)59 and the Meta-analysis Of Observational Studies in Epidemiology (MOOSE)60 in this systematic review.
Eligibility criteria
We included randomized controlled trials (RCTs) that compared TZDs against placebo/no additional drugs or other hypoglycemic agents in patients with diabetes mellitus and renal impairment. Eligible studies should report at least one of the following outcomes: (1) glucose level: glycosylated hemoglobin (HbA1c), fasting plasma glucose (FPG), (2) serum lipids and lipoproteins: triacylglycerol (TG), total cholesterol (TC), low-density lipoprotein (LDL) and high-density lipoprotein (HDL), and (3) patient-important outcomes: hypoglycemia, weight, edema, cardiovascular events (heart failure (HF), angina pectoris, myocardial infarction (MI), stroke, cardiovascular mortality) and all-cause mortality. For patient-important outcomes, we also included cohort studies and case-control studies. Renal impairment was defined according to the presence or absence of kidney damage (abnormalities in pathological, urine, blood, or imaging test) and levels of kidney function. The degree of renal impairment was classified as non-ESRD (presence of kidney damage and/or decreased kidney function, not on dialysis), and ESRD (receiving dialysis or kidney transplantation).
Literature search
A systematic literature search of PubMed, EMBASE, and Cochrane Central Register of Controlled Trials (CENTRAL) was performed from inception to 15 March 2016. We combined both MeSH and free words terms about “diabetes mellitus”, “chronic kidney disease” and “thiazolidinediones” for identifying relevant articles (Supplementary Text 1). We also screened ClinicalTrials.gov and reference lists of published reviews to identify additional relevant studies. Only studies published in English were included.
Study screening and data collection
Two authors (WW and XZ) independently screened titles/abstracts and full-text articles to identify eligibility, assessed risk of bias, and collected data from each eligible study. We used standardized, pilot-tested forms, together with detailed instructions. For the included studies, we extracted data regarding study characteristics (study design, total number of patients, length of follow up and number of patients lost to follow up), baseline characteristics (gender, age, duration of diabetes, type of renal impairment, FPG, HbA1c), intervention and outcomes of interest. Disagreement was resolved through discussion or, if required, adjudication by a third author (JSWK).
Risk of bias assessment
We assessed risk of bias of RCTs using a modified version of the Cochrane Collaboration’s tool for assessing risk of bias61, 62. The items included random sequence generation, allocation concealment, blinding of participants, caregivers, and assessors of outcomes, selective reporting, adequate follow up, and comparability.
We used the modified Newcastle-Ottawa Scale (NOS) for assessing the quality of cohort studies. We removed “representativeness of the exposed cohort” and “was follow-up long enough for outcomes to occur” as these items relate to applicability of results, and added “assessment of prognostic factors” and “similar co-interventions” to assess comparability between groups63, 64.
Data synthesis and analysis
We analyzed RCTs and observational studies separately using risk ratios (RRs) for dichotomous outcomes and mean differences (MDs) for continuous outcomes with corresponding 95% confidence intervals (CIs) to compare difference between TZDs and control groups. We pooled RRs using the Mantel-Haenszel method, and MD using the inverse variance method. Statistical heterogeneity among studies was examined by the Chi-square test and quantified by the I2 statistic65. We explored sources of heterogeneity using the following subgroup analyses: type of renal impairment (non-ESRD vs. ESRD); type of TZDs (pioglitazone vs. rosiglitazone) and type of control (placebo/no additional drugs vs. active treatment). We carried out sensitivity analyses by using alternative pooling methods (Peto vs. Mantel-Haenszel method), and statistical models regarding heterogeneity (random-effects vs. fixed-effect). We also detected publication bias by visually examining symmetry of funnel plots and Egger’s tests.
References
IDF DIABETES ATLAS. http://www.diabetesatlas.org/.
National Kidney Foundation. KDOQI Clinical Practice Guideline for Diabetes and CKD: 2012 Update. Am J Kidney Dis 60, 850–886, doi:10.1053/j.ajkd.2012.07.005 (2012).
Abe, M., Okada, K. & Soma, M. Antidiabetic agents in patients with chronic kidney disease and end-stage renal disease on dialysis: metabolism and clinical practice. Curr Drug Metab 12, 57–69, doi:10.2174/138920011794520053 (2011).
Tuttle, K. R. et al. Diabetic kidney disease: a report from an ADA Consensus Conference. Am J Kidney Dis 64, 510–533, doi:10.1053/j.ajkd.2014.08.001 (2014).
Shah, P. & Mudaliar, S. Pioglitazone: side effect and safety profile. Expert Opin Drug Saf 9, 347–354, doi:10.1517/14740331003623218 (2010).
Sarafidis, P. A., Stafylas, P. C., Georgianos, P. I., Saratzis, A. N. & Lasaridis, A. N. Effect of thiazolidinediones on albuminuria and proteinuria in diabetes: a meta-analysis. Am J Kidney Dis 55, 835–847, doi:10.1053/j.ajkd.2009.11.013 (2010).
Pfutzner, A., Schneider, C. A. & Forst, T. Pioglitazone: an antidiabetic drug with cardiovascular therapeutic effects. Expert Rev Cardiovasc Ther 4, 445–459, doi:10.1586/14779072.4.4.445 (2006).
Singh, S., Loke, Y. K. & Furberg, C. D. Long-term risk of cardiovascular events with rosiglitazone: a meta-analysis. JAMA 298, 1189–1195, doi:10.1001/jama.298.10.1189 (2007).
Nissen, S. E. & Wolski, K. Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med 356, 2457–2471, doi:10.1056/NEJMoa072761 (2007).
Habib, Z. A. et al. Relationship between thiazolidinedione use and cardiovascular outcomes and all-cause mortality among patients with diabetes: a time-updated propensity analysis. Pharmacoepidemiol Drug Saf 18, 437–447, doi:10.1002/pds.1722 (2009).
Home, P. D. et al. Rosiglitazone evaluated for cardiovascular outcomes in oral agent combination therapy for type 2 diabetes (RECORD): a multicentre, randomised, open-label trial. Lancet 373, 2125–2135, doi:10.1016/S0140-6736(09)60953-3 (2009).
Florez, H. et al. Rosiglitazone treatment and cardiovascular disease in the Veterans Affairs Diabetes Trial. Diabetes Obes Metab 17, 949–955, doi:10.1111/dom.12487 (2015).
Yokoyama, H. et al. Pioglitazone treatment and cardiovascular event and death in subjects with type 2 diabetes without established cardiovascular disease (JDDM 36). Diabetes Res Clin Pract 109, 485–492, doi:10.1016/j.diabres.2015.06.005 (2015).
Brunelli, S. M., Thadhani, R., Ikizler, T. A. & Feldman, H. I. Thiazolidinedione use is associated with better survival in hemodialysis patients with non-insulin dependent diabetes. Kidney Int 75, 961–968, doi:10.1038/ki.2009.4 (2009).
Ramirez, S. P. et al. Rosiglitazone is associated with mortality in chronic hemodialysis patients. J Am Soc Nephrol 20, 1094–1101, doi:10.1681/asn.2008060579 (2009).
Abe, M. et al. Clinical effectiveness and safety evaluation of long-term pioglitazone treatment for erythropoietin responsiveness and insulin resistance in type 2 diabetic patients on hemodialysis. Expert Opin Pharmacother 11, 1611–1620, doi:10.1517/14656566.2010.495119 (2010).
Agarwal, R. et al. A pilot randomized controlled trial of renal protection with pioglitazone in diabetic nephropathy. Kidney Int 68, 285–292, doi:10.1111/j.1523-1755.2005.00416.x (2005).
Guideline development group.. Clinical Practice Guideline on management of patients with diabetes and chronic kidney disease stage 3b or higher (eGFR <45 mL/min). Nephrol Dial Transplant 30, ii1–ii142, doi:10.1093/ndt/gfv100 (2015).
Abe, M., Kikuchi, F., Kaizu, K. & Matsumoto, K. Combination therapy of pioglitazone with voglibose improves glycemic control safely and rapidly in Japanese type 2-diabetic patients on hemodialysis. Clin Nephrol 68, 287–294, doi:10.5414/CNP68287 (2007).
Abe, M., Okada, K., Kikuchi, F. & Matsumoto, K. Clinical investigation of the effects of pioglitazone on the improvement of insulin resistance and blood pressure in type 2-diabetic patients undergoing hemodialysis. Clin Nephrol 70, 220–228, doi:10.5414/CNP70220 (2008).
Agrawal, A., Sautter, M. C. & Jones, N. P. Effects of rosiglitazone maleate when added to a sulfonylurea regimen in patients with type 2 diabetes mellitus and mild to moderate renal impairment: a post hoc analysis. Clin Ther 25, 2754–2764, doi:10.1016/S0149-2918(03)80331-4 (2003).
Arashnia, R., Roohi-Gilani, K., Karimi-Sari, H., Nikjoo, N. & Bahramifar, A. Effect of pioglitazone therapy on high sensitive C-reactive protein and lipid profile in diabetic patients with renal transplantation; a randomize clinical trial. J Nephropathol 4, 48–53, doi:10.12860/jnp.2015.10 (2015).
Banerji, M. A., Purkayastha, D. & Francis, B. H. Safety and tolerability of vildagliptin vs. thiazolidinedione as add-on to metformin in type 2 diabetic patients with and without mild renal impairment: a retrospective analysis of the GALIANT study. Diabetes Res Clin Pract 90, 182–190, doi:10.1016/j.diabres.2010.06.022 (2010).
Chan, D. T., Watts, G. F., Irish, A. B. & Dogra, G. K. Rosiglitazone does not improve vascular function in subjects with chronic kidney disease. Nephrol Dial Transplant 26, 3543–3549, doi:10.1093/ndt/gfr049 (2011).
Galle, J. et al. Comparison of the Effects of Pioglitazone versus Placebo when Given in Addition to Standard Insulin Treatment in Patients with Type 2 Diabetes Mellitus Requiring Hemodialysis: Results from the PIOren Study. Nephron Extra 2, 104–114, doi:10.1159/000337334 (2012).
Jin, H. M. & Pan, Y. Renoprotection provided by losartan in combination with pioglitazone is superior to renoprotection provided by losartan alone in patients with type 2 diabetic nephropathy. Kidney Blood Press Res 30, 203–211, doi:10.1159/000104089 (2007).
Katavetin, P., Eiam-Ong, S. & Suwanwalaikorn, S. Pioglitazone reduces urinary protein and urinary transforming growth factor-beta excretion in patients with type 2 diabetes and overt nephropathy. J Med Assoc Thai 89, 170–177 (2006).
Morikawa, A. et al. Pioglitazone reduces urinary albumin excretion in renin-angiotensin system inhibitor-treated type 2 diabetic patients with hypertension and microalbuminuria: the APRIME study. Clin Exp Nephrol 15, 848–853, doi:10.1007/s10157-011-0512-3 (2011).
Nakamura, T. et al. Effect of pioglitazone on carotid intima-media thickness and arterial stiffness in type 2 diabetic nephropathy patients. Metabolism 53, 1382–1386, doi:10.1016/j.metabol.2004.05.013 (2004).
Nakamura, T., Sugaya, T., Kawagoe, Y., Ueda, Y. & Koide, H. Effect of pioglitazone on urinary liver-type fatty acid-binding protein concentrations in diabetes patients with microalbuminuria. Diabetes Metab Res Rev 22, 385–389, doi:10.1002/dmrr.633 (2006).
Nakamura, T. et al. Pioglitazone reduces urinary podocyte excretion in type 2 diabetes patients with microalbuminuria. Metabolism 50, 1193–1196, doi:10.1053/meta.2001.26703 (2001).
Nakamura, T. et al. Comparative effects of pioglitazone, glibenclamide, and voglibose on urinary endothelin-1 and albumin excretion in diabetes patients. J Diabetes Complications 14, 250–254, doi:10.1016/S1056-8727(00)00124-0 (2000).
Pistrosch, F. et al. Effect of thiazolidinedione treatment on proteinuria and renal hemodynamic in type 2 diabetic patients with overt nephropathy. Horm Metab Res 44, 914–918, doi:10.1055/s-0032-1314836 (2012).
Wong, T. Y. et al. Rosiglitazone reduces insulin requirement and C-reactive protein levels in type 2 diabetic patients receiving peritoneal dialysis. Am J Kidney Dis 46, 713–719, doi:10.1053/j.ajkd.2005.06.020 (2005).
Yanagawa, T., Araki, A., Sasamoto, K., Shirabe, S. & Yamanouchi, T. Effect of antidiabetic medications on microalbuminuria in patients with type 2 diabetes. Metabolism 53, 353–357, doi:10.1016/j.metabol.2003.10.025 (2004).
Chen, Y. H. et al. Thiazolidinediones and Risk of Long-Term Dialysis in Diabetic Patients with Advanced Chronic Kidney Disease: A Nationwide Cohort Study. PLoS One 10, e0129922, doi:10.1371/journal.pone.0129922 (2015).
Maruthur, N. M. et al. Diabetes Medications as Monotherapy or Metformin-Based Combination Therapy for Type 2 Diabetes: A Systematic Review and Meta-analysis. Ann Intern Med 164, 740–751, doi:10.7326/M15-2650 (2016).
Dormandy, J. A. et al. Secondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial In macroVascular Events): a randomised controlled trial. Lancet 366, 1279–1289, doi:10.1016/s0140-6736(05)67528-9 (2005).
Chiquette, E., Ramirez, G. & Defronzo, R. A meta-analysis comparing the effect of thiazolidinediones on cardiovascular risk factors. Arch Intern Med 164, 2097–2104, doi:10.1001/archinte.164.19.2097 (2004).
American Diabetes Association. Standards of Medical Care in Diabetes-2016. Diabetes care 39(suppl. 1), S1–S112 (2016).
Berlie, H. D., Kalus, J. S. & Jaber, L. A. Thiazolidinediones and the risk of edema: a meta-analysis. Diabetes Res Clin Pract 76, 279–289, doi:10.1016/j.diabres.2006.09.010 (2007).
Nagajothi, N. et al. Pioglitazone and the risk of myocardial infarction and other major adverse cardiac events: a meta-analysis of randomized, controlled trials. Am J Ther 15, 506–511, doi:10.1097/MJT.0b013e318167180c (2008).
Mannucci, E., Monami, M., Lamanna, C., Gensini, G. F. & Marchionni, N. Pioglitazone and cardiovascular risk. A comprehensive meta-analysis of randomized clinical trials. Diabetes Obes Metab 10, 1221–1138, doi:10.1111/j.1463-1326.2008.00892.x (2008).
Lago, R. M., Singh, P. P. & Nesto, R. W. Congestive heart failure and cardiovascular death in patients with prediabetes and type 2 diabetes given thiazolidinediones: a meta-analysis of randomised clinical trials. Lancet 370, 1129–36, doi:10.1016/s0140-6736(07)61514-1 (2007).
Nissen, S. E. & Wolski, K. Rosiglitazone revisited: an updated meta-analysis of risk for myocardial infarction and cardiovascular mortality. Arch Intern Med 170, 1191–1201, doi:10.1001/archinternmed.2010.207 (2010).
Kernan, W. N. et al. Pioglitazone after Ischemic Stroke or Transient Ischemic Attack. N Engl J Med 374, 1321–1331, doi:10.1056/NEJMoa1506930 (2016).
Halcox, J. P. et al. Prognostic value of coronary vascular endothelial dysfunction. Circulation 106, 653–658, doi:10.1161/01.CIR.0000025404.78001.D8 (2002).
Werner, N. et al. Circulating endothelial progenitor cells and cardiovascular outcomes. N Engl J Med 353, 999–1007, doi:10.1056/NEJMoa043814 (2005).
Chen, R., Yan, J., Liu, P. & Wang, Z. Effects of thiazolidinedione therapy on inflammatory markers of type 2 diabetes: a meta-analysis of randomized controlled trials. PloS one 10, e0123703, doi:10.1371/journal.pone.0123703 (2015).
Mizoguchi, M. et al. Pioglitazone attenuates atherosclerotic plaque inflammation in patients with impaired glucose tolerance or diabetes a prospective, randomized, comparator-controlled study using serial FDG PET/CT imaging study of carotid artery and ascending aorta. JACC Cardiovascular imaging 4, 1110–1118, doi:10.1016/j.jcmg.2011.08.007 (2011).
Calnek, D. S., Mazzella, L., Roser, S., Roman, J. & Hart, C. M. Peroxisome proliferator-activated receptor gamma ligands increase release of nitric oxide from endothelial cells. Arterioscler Thromb Vasc Biol 23, 52–57, doi:10.1161/01.ATV.0000044461.01844.C9 (2003).
Werner, C., Kamani, C. H., Gensch, C., Bohm, M. & Laufs, U. The peroxisome proliferator-activated receptor-gamma agonist pioglitazone increases number and function of endothelial progenitor cells in patients with coronary artery disease and normal glucose tolerance. Diabetes 56, 2609–2615, doi:10.2337/db07-0069 (2007).
Martens, F. M., Visseren, F. L., de Koning, E. J. & Rabelink, T. J. Short-term pioglitazone treatment improves vascular function irrespective of metabolic changes in patients with type 2 diabetes. J Cardiovasc Pharmacol 46, 773–778, doi:10.1097/01.fjc.0000187176.13403.05 (2005).
Forst, T. et al. Influence of glucose control and improvement of insulin resistance on microvascular blood flow and endothelial function in patients with diabetes mellitus type 2. Microcirculation 12, 543–50, doi:10.1080/10739680500253402 (2005).
Wohrle, J. et al. Impact of pioglitazone on coronary endothelial function in non-diabetic patients with coronary artery disease. Clin Res Cardiol 97, 726–733, doi:10.1007/s00392-008-0663-8 (2008).
Loke, Y. K., Kwok, C. S. & Singh, S. Comparative cardiovascular effects of thiazolidinediones: systematic review and meta-analysis of observational studies. BMJ 342, d1309, doi:10.1136/bmj.d309 (2011).
Nissen, S. E. et al. Comparison of pioglitazone vs glimepiride on progression of coronary atherosclerosis in patients with type 2 diabetes: the PERISCOPE randomized controlled trial. JAMA 299, 1561–1573, doi:10.1001/jama.299.13.1561 (2008).
Gerstein, H. C. et al. Effect of rosiglitazone on progression of coronary atherosclerosis in patients with type 2 diabetes mellitus and coronary artery disease: the assessment on the prevention of progression by rosiglitazone on atherosclerosis in diabetes patients with cardiovascular history trial. Circulation 121, 1176–1187, doi:10.1161/circulationaha.109.881003 (2010).
Moher, D., Liberati, A., Tetzlaff, J. & Altman, D. G. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339, b2535, doi:10.1136/bmj.b2535 (2009).
Stroup, D. F. et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 283, 2008–2012, doi:10.1001/jama.283.15.2008 (2000).
Higgins, J., Green, S. The Cochrane Collaboration.Cochrane handbook for systematic reviews of interventions version 5.1.0. 2011. http://handbook.cochrane.org/.
Guyatt, G. H., Busse, J. W. Tool to Assess Risk of Bias in Randomized Controlled Trials. https://distillercer.com/resources/.
Wells, G. A. et al. University of Ottawa. The Newcastle Ottawa Scale (NOS) for assessing the quality of non randomised studies in Meta analyses. (2011). http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
Guyatt, G. H., Busse, J. W. Tool to Assess Risk of Bias in Cohort Studies. https://distillercer.com/resources/.
Higgins, J. P. & Thompson, S. G. Quantifying heterogeneity in a meta-analysis. Stat Med 21, 1539–1558, doi:10.1002/sim.1186 (2002).
Acknowledgements
We thank Jiajie Yu for assistance with the study design, and Jianrong Chen for important contribution in study screening. This study was supported by the National Natural Science Foundation of China (Grant No. 71573183), “Thousand Youth Talents Plan” of China (Grant No. D1024002) and Sichuan Province, and Young Investigator Award of Sichuan University (Grant No. 2013SCU04A37). These funders had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Author information
Authors and Affiliations
Contributions
Research idea and study design: W.W., X.Z., X.S.; data acquisition: W.W., X.Z.; data analysis/interpretation: W.W., X.Z., J.S.W.K., L.L.; statistical analysis: W.W., X.Z., J.S.W.K., L.L.; supervision or mentorship: Y.P.L., X.S. Each author contributed important intellectual content during manuscript drafting or revision and accepts accountability for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved. W.W. and X.S. take responsibility that this study has been reported honestly, accurately and transparently; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
41598_2017_1965_MOESM1_ESM.pdf
Efficacy and safety of thiazolidinediones in diabetes patients with renal impairment: a systematic review and meta-analysis
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wang, W., Zhou, X., Kwong, J.S.W. et al. Efficacy and safety of thiazolidinediones in diabetes patients with renal impairment: a systematic review and meta-analysis. Sci Rep 7, 1717 (2017). https://doi.org/10.1038/s41598-017-01965-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-01965-0
This article is cited by
-
Utility of Hypoglycemic Agents to Treat Asthma with Comorbid Obesity
Pulmonary Therapy (2023)
-
2023 UPDATE: Luso-Brazilian evidence-based guideline for the management of antidiabetic therapy in type 2 diabetes
Diabetology & Metabolic Syndrome (2023)
-
Portuguese-Brazilian evidence-based guideline on the management of hyperglycemia in type 2 diabetes mellitus
Diabetology & Metabolic Syndrome (2020)
-
Comparison of Oral Antidiabetic Drugs as Add-On Treatments in Patients with Type 2 Diabetes Uncontrolled on Metformin: A Network Meta-Analysis
Diabetes Therapy (2018)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
