
Abstract
Background:
Enhanced stimulation of the lower gut is hypothesized to play a key role in the weight loss and resolution of diabetes following bariatric surgeries. Ileal transposition (IT) permits study of the effects of direct lower gut stimulation on body weight, glucose homeostasis and other metabolic adaptations without the confounds of gastric restriction or foregut exclusion. However, the underlying mechanisms and the length of the ileum sufficient to produce metabolic benefits following IT surgery remain largely unknown.
Objective:
To determine the effects of transposing varying lengths of the ileum to upper jejunum on food intake, body weight, glucose tolerance and lower gut hormones, and the expression of key markers of glucose and lipid metabolism in skeletal muscle and adipose tissue in rats.
Methods:
Adult male Sprague–Dawley rats (n=9/group) were subjected to IT surgery with translocation of 5, 10 or 20 cm of the ileal segment to proximal jejunum or sham manipulations. Daily food intake and body weight were recorded, and an intraperitoneal glucose tolerance test was performed. Blood samples were assayed for hormones and tissue samples for mRNA (RT–qPCR) and/or protein abundance (immunoblotting) of regulatory metabolic markers.
Results:
We demonstrate that IT surgery exerts ileal length-dependent effects on multiple parameters including: (1) decreased food intake and weight gain, (2) improved glucose tolerance, (3) increased tissue expression and plasma concentrations of glucagon-like peptide-1 (GLP-1) and peptide YY (PYY), and decreased leptin concentrations and (4) upregulation of key markers of glucose metabolism (glucose transporter-4 (GLUT-4), insulin receptor substrate 1 (IRS-1), adenosine monophosphate-activated protein kinase (AMPK), hexokinase (HK) and phosphofructokinase (PFK)) together with a downregulation of lipogenic markers (fatty acid synthase (FAS)) in muscle and adipose tissue.
Conclusions:
Together, our data demonstrate that the reduction in food intake and weight gain, increase in lower gut hormones, glycemic improvements and associated changes in tissue metabolic markers following IT surgery are dependent on the length of the transposed ileum.
Similar content being viewed by others

Introduction
The International Diabetes Federation Taskforce on Epidemiology and Prevention of Diabetes recommends bariatric surgery as a treatment option for obese diabetics (BMI⩾35) and as an alternative treatment option for moderately obese subjects (BMI 30–35) with poorly controlled diabetes.1 Roux-en-Y gastric bypass, a reference standard for bariatric procedures, is hypothesized to produce weight loss and improve diabetic control through multiple mechanisms, including gastric restriction, exclusion of the foregut, enhanced lower gut stimulation due to delivery of partially digested food to the ileum and lower intestine, malabsorption, increased energy expenditure and/or improvements in insulin sensitivity in peripheral tissues;2, 3, 4 the relative importance of these mechanisms is unknown. Importantly, the improvements in diabetes and other co-morbidities of obesity appear to be dissociated from the surgery-induced weight loss.2, 3, 4, 5, 6 However, the mechanism(s) of diabetes resolution following bariatric surgeries remains poorly understood.
Bariatric surgeries involve manipulations of the foregut and/or hindgut. Ileal transposition (IT) surgery is exclusively a hindgut procedure and involves translocation of a segment of the ileum proximally into the upper jejunum without altering the length of the gastrointestinal tract or gastric restriction.7, 8 Thus, IT permits study of the effects of early exposure of the ileum to undigested nutrients on - food intake, body weight and metabolic adaptations without confounds of gastric restriction or foregut exclusion. In humans, a combination of IT with sleeve gastrectomy was shown to produce significant remission of diabetes with improvements in other co-morbidities of obesity.9, 10, 11 The length of the transposed ileum required to achieve optimal weight loss and metabolic benefits has not been completely characterized. Transposition of a 10 or 20 cm length of ileal segment in rats was shown to decrease food intake and weight gain in some studies,7, 8, 12, 13, 14, 15, 16, 17 whereas transposition of a 10 cm ileal segment was shown to have no effect on these parameters in other reports.18, 19, 20, 21, 22 These inconsistencies among studies could likely be due to differences in animal models, degree of adiposity and/or diabetic status. Interestingly, transposition of 10 cm of the ileum to the duodenum was found to produce significant improvements in glycemic control independent of weight loss in rat models.15, 18, 19, 22, 23, 24 It remains to be determined whether the magnitude of improvements in glucose tolerance is dependent on the length of the transposed ileum.
Koopmans12, 25, 26 and Atkinson8, 27, 28 postulated that expedited nutrient delivery to the lower gut would generate signals that play a key role in the long-term regulation of food intake and body weight. Consistent with this lower gut hypothesis, we16, 29 and others12, 15, 17, 18, 19, 21, 22, 24, 30 have shown that IT surgery leads to enhanced secretion of the anorexigenic lower gut hormones, glucagon-like peptide-1 (GLP-1) and peptide YY (PYY), in rats. Systemic administration of a GLP-1 receptor antagonist has been shown to attenuate the improvements in glucose homeostasis following IT surgeries31 supporting a direct role for GLP-1 in glycemic improvements; however, the role of peripheral tissues in such diabetic improvements remains largely unknown.
Skeletal muscle, liver and adipose tissues account for about 80, 5 and 1% of total glucose metabolized, respectively, in humans,32 with ectopic lipid deposition contributing to impaired insulin signaling and diabetes.33 Improvements in glucose and lipid metabolism following weight loss interventions are often associated with increased glucose uptake and clearance by muscle, adipose and liver tissues, decreased lipogenesis in peripheral tissues and/or enhanced lipid oxidation in muscle. Roux-en-Y gastric bypass was found to increase the protein content of insulin receptors, insulin receptor substrates (IRS-1, IRS-2) and the insulin-sensitive glucose transporter-4 (GLUT-4)34 in the skeletal muscle of rats. Similarly, IT was shown to increase glucose uptake,19 as well as GLUT-4 and IRS-1 protein abundance in cardiac muscle of rats;35 however, it is unknown whether IT affects other regulatory molecules of glucose and lipid metabolism in skeletal muscle and adipose tissue. Thus, despite some evidence for a role for muscle in the metabolic effects of surgeries, the underlying molecular mechanisms mediating improvements in glucose and lipid homeostasis following bariatric surgeries are poorly understood. Therefore, to understand the mechanisms by which IT surgeries promote weight loss and glycemic improvements, we compared the ‘size-dependent’ effects of transposing varying lengths of the ileum (5, 10 or 20 cm) to the upper jejunum on multiple parameters, including food intake, body weight, glucose tolerance, lower gut hormones and key markers of glucose and lipid metabolism in skeletal muscle and adipose tissue in rats.
Materials and methods
Animals
All animal experimentation was conducted in accordance with the regulations of the Canadian Council of Animal Care and was approved by the Animal Care Committee of the University of Calgary. Male Sprague–Dawley rats (Charles River, Montreal, QC, Canada) that weighed ∼400 g were housed individually in wire mesh cages in a room with a controlled temperature environment (19–21 °C) and a 12:12 h light:dark cycle (dark onset at 1000 h). The animals were provided a pelleted rat chow (Labdiet, PROLAB RMH2500 Rodent diet, PMI Nutrition International, LLC, St Louis, MO, USA) and water ad libitum and were allowed to adapt to the environmental conditions for at least two weeks before experimentation.
Surgical model
The animals were provided daily a fresh complete mixed nutrient liquid diet Ensure Plus (57%, 15% and 28% calories from carbohydrate, protein and fat, respectively; 1.5 kcal ml−1; Abbott Laboratories, Saint-Laurent, QC, Canada). The Ensure Plus diet was initiated 3–4 days prior to the surgeries to allow adaptation to liquid diets and subsequently continued to be fed throughout the study. Before the surgeries, the animals were fasted for ∼12 h but had ad libitum access to water. Surgeries were performed under isoflurane anaesthesia (2–4%; 1 L per minute O2 flow) with administration of an antibiotic (Baytril Bayer HealthCare, Toronto, ON, Canada), analgesic (Buprenorphine) and saline (Baxter, Mississauga, ON, Canada) during the preoperative period and at ∼12 h intervals for 48 h postoperatively. The rats (430–560 g) were randomly assigned to one of four surgical procedures (n=9 per group): sham, 5 cm IT, 10 cm IT or 20 cm IT, with the IT surgeries performed as we described previously.16, 29 Briefly, a segment of the ileum measuring 5 cm, 10 cm or 20 cm, located 20 cm proximal to the cecum, was resected and then transposed in the same orientation to the proximal jejunum at ∼5 cm distal to the ligament of Treitz. The sham operations involved intestinal transections, followed by reanastomosis at three locations: 5 cm distal to the ligament of Treitz and at 20 and 40 cm proximal to the cecum.
Food intake and body weight
Daily food intake (23 h) and body weight were recorded between 0900–1000 h. At onset of dark period (1000 h), the animals were provided daily a fresh complete mixed nutrient liquid diet Ensure Plus. Mixed nutrient liquid diets were originally used to characterize the effects of IT surgeries on intake and gut hormones in rat models.12 We showed that, when given access to a high-fat solid diet and Ensure plus liquid diet, rats consume 80% of their total calories from Ensure.36 Therefore, Ensure Plus liquid diet was used in the current study because it permits comparisons with previous studies, is highly palatable for rats, allows for more rapid passage of food across the sites of anastomosis with minimal blockage, and liquid diets permit more precise recording of intakes with relatively less spillage. We previously used this mixed nutrient liquid diet to compare the effects of IT and Roux-en-Y gastric bypass surgeries on food intake and body weight,16 and recently demonstrated that with Ensure feeding adult male Sprague–Dawley rats rapidly gained weight and were glucose intolerant when compared to age-matched chow fed animals.29 Further, similar to our model, numerous recent studies characterized the anorexic, weight loss and other metabolic effects of bariatric surgeries using non-obese rats37, 38, 39, 40, 41, 42, 43, 44 that were maintained completely on a mixed nutrient liquid diet following surgical interventions.45
Intraperitoneal glucose tolerance test
At 4 weeks into the postoperative period, following an overnight fast, all animals were subject to an intraperitoneal injection of 50% dextrose at 2 g per kg body weight. Tail vein blood glucose concentrations were determined using a hand-held glucose meter (Accu-Chek glucose meter, Roche Diagnostics, QC, Canada) at baseline (0), 30, 60 and 120 min after dextrose injection.
Blood and tissue sampling
Following completion of behavioural measures, at 4-weeks post-surgery, all rats were subjected to tail-vein blood sampling after overnight fasting as we described previously.16, 29 Briefly, the fasted animals were allowed to consume ∼8 ml of Ensure over a 15 min period, and blood samples were collected at baseline (0) and 60 min after complete consumption of the mixed-nutrient liquid meal Ensure Plus. Blood samples were collected on ice in tubes containing EDTA (1 mg ml−1 blood) and a cocktail of enzyme inhibitors (DPP-IV inhibitor (10 μl ml−1 blood; Millipore Corporation, Billerica, CA, USA) and protease inhibitor cocktail (10 μl ml−1 blood; Sigma, St Louis, MO, USA)), centrifuged at 1000 × g for 10 min at 4 °C within 30 min of blood collection, and finally the plasma was separated and stored at −80 °C until analysis. The animals were then euthanized (Euthanyl, Bimeda MTC Animal Health, Cambridge, ON, Canada) and representative samples of the epididymal fat and a mixed leg muscle were collected, rinsed in sterile saline, snap frozen in liquid nitrogen and stored at −80 °C. Further, a segment of the transposed ileum in IT rats, and a comparable ileal segment in sham rats, were collected, rinsed in sterile saline and bisected with one fragment fixed in 10% formalin and the remainder snap frozen in liquid nitrogen and stored at −80 °C.
Hormone assays
Plasma PYY and GLP-1 concentrations were quantified by enzyme-linked immunosorbent assays (S-1274, S-1359, Bachem Americas Inc., Torrance, CA, USA) following the instructions of the manufacturer. The PYY assay (S-1274) cross reacts with both PYY (1-36) and PYY (3-36), and the intra-assay was 5.2%. The GLP-1 assay (S-1359) cross reacts with GLP-1 (7-36) and GLP-1 (7-37), and the intra-assay CV was 2.8%. Plasma concentrations of insulin and leptin were measured using a Milliplex rat gut hormone panel (Milliplex, Millipore; Luminex Crp., Austin, TX, USA) on a Luminex platform (Bio-Plex 200) with intra-assay CV of 5.4% and 6.2%, respectively.
RNA isolation and real time qPCR
For RNA isolation, 100−300 mg of frozen tissue (fat, muscle or ileum) was homogenized (AHS200 PowerMax, VWR, Mississauga, ON, Canada) in QIAzol Lysis Reagent (Qiagen, Gaithersburg, MD, USA) and mRNA isolated using the Qiagen RNeasy Lipid Tissue Mini kit following the instructions of the manufacturer (Qiagen, Toronto, ON, Canada). The RNA concentration was measured with a NanoDrop ND-1000 spectrophotometer (Thermo Fisher Scientific Inc., Mississauga, ON, Canada), and only samples with a 260:280 ratio of 1.9−2.1 were used in the current study. The cDNA synthesis and qPCR were performed on an Mastercycler ep realplex thermocycler (Eppendorf, Mississauga, ON, Canada) with reagents from Life Technologies (Burlington, ON, Canada) following previously reported procedures.29, 46 All PCR conditions were optimized for primer concentration and annealing temperatures (Supplementary Table 1); amplification efficiency ranged between 85−110%. RT–qPCR was then performed on the following genes of interest: peptide-YY (PYY) and preproglucagon in the gut, acetyl-CoA carboxylase, fatty acid synthase (FAS), carnitine palmitoyl transferase-1b (CPT-1b), hormone sensitive lipase, GLUT-4, hexokinase 1 (HK) and phosphofructokinase muscle (PFK) in adipose tissue and muscle, using β-actin as an internal housekeeping gene. Relative quantification was then performed by the ΔΔCt method using the equation: Rq=2−(ΔCp sample – ΔCp control).47, 48
Immunohistochemistry
Immunohistochemical procedures for the ileal segments was done, as we described previously,29 using commercially available antibodies for GLP-1 (sc-57166, Santa Cruz Biotechnologies, Santa Cruz, CA, USA) and PYY (ab-22663, AbCam, Cambridge, MA, USA). Following immunostaining, slides were visualized under a 20X objective of a light microscope (Olympus BX51, Center Valley, PA, USA), and the numbers of positively stained cells per villi were counted on 10 villi per section using 3 sections per animal. Villus length, villus width and crypt depth were also measured on 5 contiguous villi on three separate tissue sections, and these measures were used to estimate the histological surface magnification ratio as an index of the mucosal surface area.49
Immunoblotting
Frozen muscle tissues were homogenized and sonicated in ice-cold NP40 buffer containing protease inhibitor cocktail (P2714, Sigma-Aldrich) and 1 mM PMSF. The samples were centrifuged for 15 min at 2500 g at 4 °C to remove debris. Protein concentration in the supernatant was determined by Bradford assay (Bio-Rad Laboratories Ltd., Mississauga, ON, Canada) and standardized to 2 μg ml−1. Samples were diluted 1:2 with Laemmli buffer (S3401, Sigma-Aldrich), boiled for 4 min at 95 °C (cytoplasmic proteins), loaded (20 μg) randomly on a 10% acrylamide gel and subjected to SDS PAGE at 130 V for 1 h in a Bio-Rad gel apparatus (Mini PROTEAN Tetra Cell, 165–8000) followed by electro transfer to a nitrocellulose membrane at 100 V for 90 min. Blots were washed in TBST buffer (3 × 15 min), blocked in 5% milk (1 h) and incubated overnight in the following primary antibodies: GLUT-4 (1:500 dilution; ab654, AbCam), IRS-1 (1:1000; ab52167, AbCam), IRS-1 ser636p (1:1000; ab47764, AbCam), AMPK (1:1000; 2793 S, New England Biolabs, Ltd., Whitby, ON, Canada), GLP-1 R (1:1000; sc-66911, Santa Cruz Biotechnologies) and internal loading control β-actin (1:1000; sc-47778, Santa Cruz biotechnologies). Blots were washed again in TBST (3 × 15 min) before incubation in secondary antibody for 1 h at 4 °C (1:5000 dilution mouse anti-rabbit; 211-032-171, Jackson Immunoresearch, West Grove, PA, USA) or donkey anti-mouse for AMPK (1:2500; 715-066-150, Jackson Immunoresearch). Blots were visualized with ECL illumination (Lumi-light western blotting substrate, Roche Diagnostics, Mannheim, Germany) and band intensities quantified on a ChemiDoc MP system using Image J software (Bio-Rad Laboratories Ltd.).
Statistical analyses
Daily food intake, body weight and glucose tolerance data were analyzed by repeated-measures ANOVA or ANOVA followed by Dunnett’s post-hoc test using SPSS (IBM, Markham, ON, Canada). Data on plasma hormone concentrations, area under the curve, gut immunohistochemistry, qPCR and relative protein abundance by immunoblotting were analyzed using one-way ANOVA followed by Dunnett’s post-hoc test. Significance was declared at P<0.05 and trends at P<0.10. All data are presented as mean±s.e.m.
Results
Food intake and body weight
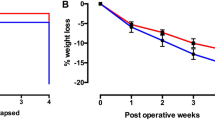
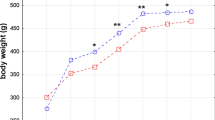
IT surgeries produced a significant reduction in food intake for 2–3 wks after surgery (Figure 1a; treatment x time, F3, 22=5.37, P<0.01). When compared to control-sham rats, food intake of the 5–20 cm IT groups was decreased by 26–36% at 1 wk (P<0.05) and by 36–39% at 2 wks (P<0.01) into the post-operative period. By 3 wks after surgery, food intake of only the 20 cm IT group was decreased by 32% (P<0.05). Mean preoperative body weight did not differ among treatments (Sham 444±18 g, 5 cm IT 451±14 g, 10 cm IT 445±10 g and 20 cm IT 458±11 g). The sham animals continued to gain weight, whereas IT surgeries prevented weight gain (Figure 1b; treatment x time, F3, 64=6.023, P<0.001). Compared to control-sham rats, weights of the 5–20 cm IT groups were decreased by 15–22% for 3 wks into the post-operative period (P<0.05). At study termination (4 wks), body weights of the sham (567±16 g) and 5 cm IT (500±15 g) groups did not differ (P>0.10), whereas the weights were decreased by 15% in the 10 cm (460±28 g; P<0.01) and 25% in the 20 cm (427±16 g; P<0.001) IT groups.

Effects of ileal transposition surgeries on food intake and body weight. Daily food intake (a) and body weight (b) of rats (n=9/group) subjected to either sham control (○, Sham) surgeries or ileal transposition (IT) surgeries in which a segment of the ileum measuring 5 cm (Δ, IT5), 10 cm (◊, IT10) or 20 cm (□, IT20) is transposed to upper jejunum. All animals subjected to surgical interventions were fed Ensure Plus liquid diet. Values are mean±s.e.m. *P<0.05 compared to sham-controls.
Intraperitoneal glucose tolerance test
IT surgery resulted in significant improvement in intraperitoneal glucose tolerance test at study termination (Figure 2; treatment x time, F3, 78=2.083, P<0.05). Blood glucose concentrations were decreased at baseline by 18–21% in the 10 and 20 cm IT groups (P<0.05), at 30 min by 35% in the 5 cm IT (P<0.05), and at 60–120 min by 24–28% in 20 cm IT (P<0.05). Further, the AUC analysis revealed a 15–25% decrease in the 5–20 cm IT groups (P<0.05).

Effects of ileal transposition surgeries on glucose tolerance. Blood glucose concentrations (a) and area under the curve (AUC) for glucose (b) following an intraperitoneal glucose tolerance test in rats (n=9/group) subjected to either sham control (○, Sham) surgeries or ileal transposition (IT) surgeries in which a segment of the ileum measuring 5 cm (Δ, IT5), 10 cm (◊, IT10) or 20 cm (□, IT20) is transposed to upper jejunum. Values are mean±s.e.m. *P<0.05 compared to sham-controls.
Gut histomorphometry and gut peptides
At termination, histomorphometry of transposed or comparable ileal segments revealed a significant increase in villus height and width in all transposed segments and an increase in crypt depth in the 5 and 20 cm ileal groups relative to control-sham rats (Supplementary Table 2, Figure 1). The histological surface index increased significantly by 20–40% in the 10–20 cm IT groups compared to control-sham.
IT resulted in a consistent elevation in GLP-1 and PYY at the level of mRNA (RT–qPCR), protein abundance (immunostaining) in the gut and plasma concentrations (Figure 3, Supplementary Figure 1). Preproglucagon mRNA was elevated 14 fold in the 20 cm IT (P<0.05), the number of immunopositive GLP-1 cells were increased 181–537% in the 10 and 20 cm IT groups (P<0.05), and postprandial plasma concentrations were elevated by 142–143% in the 10 and 20 cm IT groups (P<0.01). Similarly, PYY mRNA was elevated 16–36 fold in the 10 and 20 cm IT groups (P<0.05), the number of PYY immunopositive cells were increased 62–194% in the 5–20 cm IT groups (P<0.001) and postprandial plasma concentrations were increased 956–1392% in the 10–20 cm IT groups (P<0.05). Plasma insulin concentrations did not differ (P>0.10) among treatments (Figure 4a). Plasma leptin concentrations were decreased by 51–64% in the 10–20 cm (P<0.01) groups at baseline and postprandial concentrations decreased by 44% in the 5 cm (P<0.01), 61% in the 10 cm (P<0.001) and 83% in the 20 cm IT (P<0.001) groups (Figure 4b).

Effects of ileal transposition surgeries on glucagon-like peptide-1 (GLP-1) and peptide YY (PYY) expression and secretion. Preproglucagon mRNA abundance (a), relative numbers of GLP-1 immunopositive cells (b), plasma GLP-1 concentrations (c), PYY mRNA abundance (d), relative numbers of PYY immunopositive cells (e) and plasma PYY concentrations (f) are shown. The mRNA abundance and immunoreactivity to GLP-1 and PYY were determined in the transposed ileum of rats subjected to transposition of 5 cm (IT 5 cm), 10 cm (IT 10 cm) or 20 cm (IT 20 cm) of an ileal segment to upper jejunum, or in a comparable ileal segment of rats subjected to sham control (Sham) manipulations. At 4 weeks after surgeries, plasma GLP-1 and PYY concentrations were determined at baseline (0 min) and 60 min after consumption of a mixed nutrient liquid meal (Ensure Plus). Values are mean±s.e.m. *P<0.05, aP<0.10, when compared to sham-controls.

Effects of ileal transposition surgeries on plasma concentrations of insulin (a) and leptin (b). Plasma hormone concentrations were determined at baseline (0 min) and 60 min after consumption of a mixed nutrient liquid meal (Ensure Plus) in rats subjected to either sham-control surgeries (Sham) or ileal transposition (IT) surgeries in which a segment of the ileum measuring 5 cm (IT5), 10 cm (IT10) or 20 cm (IT20) is transposed to upper jejunum. Values are mean±s.e.m. *P<0.05, when compared to sham-controls.
Markers of glucose and lipid metabolism in muscle
IT surgeries produced significant changes in the abundance of key glucose and lipid metabolism markers in skeletal muscle (Figures 5 and 6). IT increased muscle GLUT4 at both the mRNA and protein levels (Figures 5a and b). GLUT4 mRNA abundance was elevated approximately two-fold in the 20 cm IT (P<0.05) and protein abundance increased 91% in the 20 cm IT (P<0.05). Despite a numerical 29% increase in the 20 cm IT group, GLP-1R protein abundance did not differ among treatments (Figure 5c; P>0.10). In the 20 cm IT, protein abundance of IRS-1 (Figure 5d) was increased 519% (P<0.05), whereas IRS-1 ser636p (Figure 5e) was decreased by 57% (P<0.05) and AMPK (Figure 5f) was elevated by 198% (P<0.05).

Effects of ileal transposition surgeries on relative mRNA and/or protein abundance of key markers of glucose metabolism in skeletal muscle. RT–qPCR and immunoblotting were performed on muscle samples collected at study termination from rats subjected to either sham-control (Sham) surgeries or ileal transposition (IT) surgeries in which a segment of the ileum measuring 5 cm (IT 5 cm), 10 cm (IT 10 cm) or 20 cm (IT 20 cm) is transposed to upper jejunum. The relative abundance of (a) glucose transporter-4 (GLUT-4) mRNA, (b) GLUT-4 protein, (c) glucagon-like peptide-1 receptor (GLP-1R) protein, (d) insulin receptor substrate -1 (IRS-1) protein, (e) IRS-1 phosphorylated at serine 636 (IRS-1 pS636) protein and (f) 5′ adenosine monophosphate-activated protein kinase-α (AMPKα) protein are shown. Values are mean±s.e.m. *P<0.05, when compared to sham-controls.

Effects of ileal transposition surgeries on relative mRNA abundance of key markers of glucose and lipid metabolism in muscle (a–d) and adipose tissues (e–h). RT–qPCR was performed on tissue samples collected at study termination from rats subjected to either sham-control (Sham) surgeries or ileal transposition (IT) surgeries in which a segment of the ileum measuring 5 cm (IT 5 cm), 10 cm (IT 10 cm) or 20 cm (IT 20 cm) is transposed to upper jejunum. The relative mRNA abundance of (a, e) hexokinase, (b, f) phophofructokinase (PFK), (c, g) fatty acyl synthase (FAS) and (d, h) carnitine-palmitoyl transferase-1 (CPT-1) are shown. Values are mean±s.e.m. *P<0.05, when compared to sham-controls.
Quantification of mRNA transcripts revealed significant effects of IT surgeries on key markers of glucose and lipid metabolism in muscle (Figure 6). The relative mRNA abundance of hexokinase was increased two-fold in the 20 cm IT (Figure 6a; P<0.01) and that of PFK was increased three-fold in the 20 cm IT (Figure 6b; P<0.05). We also observed a 70–97% reduction of FAS mRNA in the 10–20 cm IT groups (Figure 6c; P<0.01) and an approximately threefold elevation of CPT-1 mRNA in the 10–20 cm IT groups (Figure 6d; P<0.05).
Markers of glucose and lipid metabolism in adipose tissue
IT surgeries produced significant changes in the relative mRNA abundance of key glucose and lipid metabolism markers in adipose tissue (Figure 6). Similar to muscle, the mRNA abundance of GLUT-4 was increased 2–3 fold (P<0.01) in the 10–20 cm IT groups (Sham 1.00±0.20, 5 cm IT 0.91±0.14, 10 cm IT 2.28±0.29, 20 cm IT 2.71±0.24). Among other markers of glucose metabolism, in the 10–20 cm IT groups hexokinase mRNA was increased 3–4 fold (Figure 6e; P<0.05) and PFK mRNA was elevated 2–3 fold (Figure 6f; P<0.05). Among the lipid metabolism markers, FAS mRNA was decreased to nearly a tenth of sham levels in all groups (Figure 6g; P<0.001), whereas CPT-1 mRNA was increased by about 3–8 fold in the 5–20 cm IT groups (Figure 6h; P<0.01).
Discussion
Bariatric surgeries often lead to profound improvements in diabetes even before there is significant weight loss; the underlying mechanisms mediating improvements in glucose and lipid homeostasis are poorly understood. IT surgery offers a powerful model to discern the direct effects of lower gut stimulation alone on energy balance and metabolic improvements. Although rat models of IT are frequently used, it is unknown whether the metabolic responses are dependent on the length of the transposed ileum. We provide evidence in a rat model that IT surgery exerts effects on multiple hormonal and metabolic parameters, which are dependent on the length of the transposed ileum. These effects include: (1) reduction in food intake and weight gain, (2) improvements in intraperitoneal glucose tolerance, (3) increased tissue expression and plasma concentrations of GLP-1 and PYY and a decrease in plasma leptin concentrations, and (4) upregulation of markers of glucose metabolism (GLUT-4, IRS-1, AMPK, HK, PFK) together with a downregulation of lipogenic markers (FAS) in muscle and adipose tissue.
In the current study, the IT-induced reduction of food intake and weight gain appeared to be length-dependent. The anorexic effects of the 5–10 cm IT group lasted 2 wks and those of the 20 cm IT group for 3 wks. Further, relative to controls, the body weights of the 5 cm group were decreased for 3 wks and those of the 10–20 cm IT groups for 4 wks. Consistent with these findings, we previously showed that the reduction of weight gain lasts longer than the duration of food intake inhibition following 20 cm IT surgery in rats.16 The prolonged inhibition of weight gain despite relatively transient effects on food intake by IT could likely be due to malabsorption and/or increased energy expenditure. IT surgeries were reported to produce negligible malabsorption14, 15 but to increase energy expenditure.50 Therefore, in our study, it is likely that IT-induced stimulation of energy expenditure contributed to the reduction in weight gain beyond the transient anorexia. Previous studies on IT surgeries in rodents have reported variable findings with either a significant reduction in intake and weight gain7, 8, 12, 13, 14, 15, 16, 17, 51 or no effect on these parameters.18, 21 These inconsistencies are likely due to varying lengths of transposed ileal segments and animal models. Transposition of a 20 cm ileal segment decreased intake and weight gain,12, 16, 17 whereas transposition of shorter 10 cm lengths of ileum either had no effect18, 19, 20, 21, 22 or decreased food intake and weight gain in rats.12, 14, 15 The degree of adiposity also appears to play a role with IT producing a sustained reduction in food intake and weight gain in obese rats,7, 8, 13, 14, 15, 17 but not in diabetic rats.18, 20, 21, 22 Importantly, despite differential effects on the magnitude and duration of reduction in food intake and weight gain, all IT groups in the current study produced comparable improvements in glucose tolerance. Others have also shown that IT produces weight-independent improvements in glucose tolerance in rats.17, 18, 19, 20, 21, 22, 24, 30, 31 Overall, our data demonstrate that IT surgery produces an ileal length-dependent reduction in food intake and body weight, but the glycemic improvements appear to be independent of the magnitude of changes in food intake or body weight.
It has been hypothesized that early exposure of the transposed ileum to nutrient-rich chyme following IT surgeries leads to enhanced lower gut hormone secretion with a consequent reduction in food intake, body weight and improved glucose tolerance.12, 18, 19, 23 Our gut histomorphology data indicate that IT surgeries resulted in increased villus height, villus width, crypt depth as well as histological surface magnification suggestive of hypertrophic and hyperplastic changes in the ileal segments. We also demonstrate that IT surgery leads to an increase in the mRNA abundance and immunoreactivity for GLP-1 and PYY in the ileum, as well as their plasma concentrations, which are dependent on the length of the transposed ileal segment. The threshold for increase in these L-cell products appears to be 10 cm of the transposed ileum, which is similar to a previous study showing that 10–20 cm IT leads to increased plasma enteroglucagon concentrations12 and other studies on IT-induced increase in circulating GLP-1 and PYY concentrations.15, 17, 19, 22, 23, 24, 30, 31, 45, 52
Consistent with our previous findings,29 plasma insulin concentrations at 60 min after a meal did not differ among treatments; it is likely that insulin changes at other intervals might have been overlooked. However, the effects of IT surgeries on insulin concentrations were inconsistent with some studies reporting either no change17, 22 or decrease in insulin concentration in rats.12, 18, 19, 30 Plasma leptin concentrations were decreased in a length-dependent manner, which might be reflective of an IT-induced reduction in adipose reserves31 and is, in general, consistent with other reports.24, 30 Thus, our data provide evidence that the degree of lower gut stimulation with consequent expression and increase in plasma GLP-1 and PYY concentrations, as well as the reduction in plasma leptin concentrations, is dependent on the length of the ileum that is stimulated by early exposure to nutrients.
Together with IT-induced increase in glucose tolerance, we show here that the expression of GLUT-4, the insulin-sensitive glucose transporter, is increased nearly linearly in muscle and adipose tissues, which is suggestive of enhanced glucose clearance by these tissues and is consistent with our recent findings.29 We also found an increase in the tissue expression and plasma concentrations of GLP-1 and PYY. GLP-1 receptor blockade has been shown to attenuate IT-induced improvements in glucose tolerance;31 a similar role for PYY in IT-induced improvements in glucose disposal remains to be demonstrated. To gain further insights into the underlying mechanisms of glycemic improvements, we focussed on key metabolic signalling intermediaries. IT surgeries did not affect the protein abundance of GLP-1 receptor in muscle but increased the protein abundance of AMPKα—a key regulator of nutrient metabolism in muscle. Consistent with our recent findings,29 the protein abundance of IRS-1 was increased, whereas IRS-1 pS636, a negative modulator of IRS-1, was decreased with IT, suggestive of enhanced insulin sensitivity in muscle. Further, for the first time, we demonstrate that IT surgeries influence key markers of glucose and lipid metabolism in muscle and adipose tissues. In these tissues, the nearly linear increase in transcript abundance of the rate-limiting glycolytic enzymes—hexokinase and phosphofructokinase—is suggestive of enhanced glycolytic flux. The reciprocal decrease in FAS and increase in CPT-1 transcript abundance in muscle and adipose tissues are suggestive of decreased lipogenic and enhanced lipid oxidative capacities in both tissues. As ectopic lipid deposition in muscle and enhanced adipose tissue lipolysis play a key role in insulin resistance,33 our data suggest that IT surgery improves insulin sensitivity and glucose clearance in part by promoting glucose metabolism and lipid oxidation in muscle while concurrently decreasing lipogenesis in adipose tissue.
In conclusion, for the first time, we demonstrate that IT surgery produces an ileal length-dependent reduction in food intake and weight gain, stimulation of ileal adaptation, increased GLP-1 and PYY secretion, and enhanced glycemic improvements, which are supported by changes in key markers of glucose and lipid metabolism in muscle and adipose tissue. An understanding of the molecular mechanisms mediating the improvements in glucose and lipid homeostasis following bariatric surgeries may lead to the development of novel approaches for treating obesity and diabetes.
References
Dixon JB, Zimmet P, Alberti KG, Rubino F . Bariatric surgery: an IDF statement for obese Type 2 diabetes. Surg Obes Relat Dis 2011; 7: 433–447.
Goldfine AB, Shoelson SE, Aguirre V . Expansion and contraction: treating diabetes with bariatric surgery. Nat Med 2009; 15: 616–617.
Rubino F, Schauer PR, Kaplan LM, Cummings DE . Metabolic surgery to treat type 2 diabetes: clinical outcomes and mechanisms of action. Annu Rev Med 2010; 61: 393–411.
Cummings DE . Metabolic surgery for type 2 diabetes. Nat Med 2012; 18: 656–658.
Chandarana K, Batterham RL . Shedding pounds after going under the knife: metabolic insights from cutting the gut. Nat Med 2012; 18: 668–669.
Laferrere B . Diabetes remission after bariatric surgery: is it just the incretins? Int J Obes (Lond) 2011; 35: S22–S25.
Koopmans HS, Sclafani A, Fichtner C, Aravich PF . The effects of ileal transposition on food intake and body weight loss in VMH-obese rats. Am J Clin Nutr 1982; 35: 284–293.
Atkinson RL, Whipple JH, Atkinson SH, Stewart CC . Role of the small bowel in regulating food intake in rats. Am J Physiol 1982; 242: R429–R433.
DePaula AL, Stival AR, DePaula CC, Halpern A, Vencio S . Surgical treatment of type 2 diabetes in patients with BMI below 35: mid-term outcomes of the laparoscopic ileal interposition associated with a sleeve gastrectomy in 202 consecutive cases. J Gastrointest Surg 2012; 16: 967–976.
Vencio S, Stival A, Halpern A, DePaula CC, DePaula AL . Early mechanisms of glucose improvement following laparoscopic ileal interposition associated with a sleeve gastrectomy evaluated by the euglycemic hyperinsulinemic clamp in type 2 diabetic patients with BMI below 35. Dig Surg 2011; 28: 293–298.
De Paula AL, Stival AR, Halpern A, DePaula CC, Mari A, Muscelli E et al. Improvement in insulin sensitivity and beta-cell function following ileal interposition with sleeve gastrectomy in type 2 diabetic patients: potential mechanisms. J Gastrointest Surg 2011; 15: 1344–1353.
Koopmans HS, Ferri GL, Sarson DL, Polak JM, Bloom SR . The effects of ileal transposition and jejunoileal bypass on food intake and GI hormone levels in rats. Physiol Behav 1984; 33: 601–609.
Boozer CN, Choban PS, Atkinson RL . Ileal transposition surgery attenuates the increased efficiency of weight gain on a high-fat diet. Int J Obes 1990; 14: 869–878.
Chen DC, Stern JS, Atkinson RL . Effects of ileal transposition on food intake, dietary preference, and weight gain in Zucker obese rats. Am J Physiol 1990; 258: R269–R273.
Strader AD, Vahl TP, Jandacek RJ, Woods SC, D'Alessio DA, Seeley RJ . Weight loss through ileal transposition is accompanied by increased ileal hormone secretion and synthesis in rats. Am J Physiol Endocrinol Metab 2005; 288: E447–E453.
Chelikani PK, Shah IH, Taqi E, Sigalet DL, Koopmans HH . Comparison of the effects of Roux-en-Y gastric bypass and ileal transposition surgeries on food intake, body weight, and circulating peptide yy concentrations in rats. Obes Surg 2010; 20: 1281–1288.
Grueneberger JM, Fritz T, Zhou C, Meyer S, Karcz-Socha I, Sawczyn T et al. Long segment ileal transposition leads to early amelioration of glucose control in the diabetic obese Zucker rat. Wideochir Inne Tech Malo Inwazyjne 2013; 8: 130–138.
Cummings BP, Strader ADStanhope KL, Graham JL, Lee J, Raybould HE et al. Ileal interposition surgery improves glucose and lipid metabolism and delays diabetes onset in the UCD-T2DM rat. Gastroenterology 2010; 138: 2437–2446.
Culnan DM, Albaugh V, Sun M, Lynch CJ, Lang CH, Cooney RN . Ileal interposition improves glucose tolerance and insulin sensitivity in the obese Zucker rat. Am J Physiol Gastrointest Liver Physiol 2010; 299: G751–G760.
Patriti A, Facchiano E, Annetti C, Aisa MC, Galli F, Fanelli C et al. Early improvement of glucose tolerance after ileal transposition in a non-obese type 2 diabetes rat model. Obes Surg 2005; 15: 1258–1264.
Patriti A, Aisa MC, Annetti C, Sidoni A, Galli F, Ferri I et al. How the hindgut can cure type 2 diabetes. Ileal transposition improves glucose metabolism and beta-cell function in Goto-kakizaki rats through an enhanced Proglucagon gene expression and L-cell number. Surgery 2007; 142: 74–85.
Strader AD, Clausen TR, Goodin SZ, Wendt D . Ileal interposition improves glucose tolerance in low dose streptozotocin-treated diabetic and euglycemic rats. Obes Surg 2009; 19: 96–104.
Kindel TL, Yoder SM, Seeley RJ, D'Alessio DA, Tso P . Duodenal-jejunal exclusion improves glucose tolerance in the diabetic, Goto-Kakizaki rat by a GLP-1 receptor-mediated mechanism. J Gastrointest Surg 2009; 13: 1762–1772.
Kohli R, Kirby M, Setchell KD, Jha P, Klustaitis K, Woollett LA et al. Intestinal adaptation after ileal interposition surgery increases bile acid recycling and protects against obesity-related comorbidities. Am J Physiol Gastrointest Liver Physiol 2010; 299: G652–G660.
Koopmans HS, Sclafani A . Control of body weight by lower gut signals. Int J Obes 1981; 5: 491–495.
Koopmans HS . Satiety signals from the gastrointestinal tract. Am J Clin Nutr 1985; 42: 1044–1049.
Atkinson RL, Brent EL . Appetite suppressant activity in plasma of rats after intestinal bypass surgery. Am J Physiol 1982; 243: R60–R64.
Atkinson RL, Whipple JH, Atkinson SH, Stewar CC . Role of the small bowel in regulating food intake in rats. Am J Physiol 1982; 242: R429–R433.
Nausheen S, Shah IH, Pezeshki A, Sigalet DL, Chelikani PK . Effects of sleeve gastrectomy and ileal transposition, alone and in combination, on food intake, body weight, gut hormones, and glucose metabolism in rats. Am J Physiol Endocrinol Metab 2013; 305: E507–E518.
Ikezawa F, Shibata C, Kikuchi D, Imoto H, Miura K, Naitoh T et al. Effects of ileal interposition on glucose metabolism in obese rats with diabetes. Surgery 2012; 151: 822–830.
Gaitonde S, Kohli R, Seeley R . The role of the gut hormone GLP-1 in the metabolic improvements caused by ileal transposition. J Surg Res 2012; 178: 33–39.
DeFronzo RA, Jacot E, Jequier E, Maeder E, Wahren J, Felber JP . The effect of insulin on the disposal of intravenous glucose. Results from indirect calorimetry and hepatic and femoral venous catheterization. Diabetes 1981; 30: 1000–1007.
Samuel VT, Shulman GI . Mechanisms for insulin resistance: common threads and missing links. Cell 2012; 148: 852–871.
Bonhomme S, Guijarro A, Keslacy S, Goncalves CG, Suzuki S, Chen C et al. Gastric bypass up-regulates insulin signaling pathway. Nutrition 2011; 27: 73–80.
Yan Z, Chen W, Liu S, Zhang G, Sun D, Hu S . Myocardial insulin signaling and glucose transport are up-regulated in Goto-Kakizaki type 2 diabetic rats after ileal transposition. Obes Surg 2012; 22: 493–501.
Chelikani PK, Haver AC, Reidelberger RD . Intermittent intraperitoneal infusion of peptide YY(3-36) reduces daily food intake and adiposity in obese rats. Am J Physiol Regul Integr Comp Physiol 2007; 293: R39–R46.
Abegg K, Schiesser M, Lutz TA, Bueter M . Acute peripheral GLP-1 receptor agonism or antagonism does not alter energy expenditure in rats after Roux-en-Y gastric bypass. Physiol Behav 2013; 119: 92–96.
Asarian L, Abegg K, Geary N, Schiesser M, Lutz TA, Bueter M . Estradiol increases body weight loss and gut-peptide satiation after Roux-en-Y gastric bypass in ovariectomized rats. Gastroenterology 2012; 143: 325–327.
Bueter M, Ahmed A, Ashrafian H, Le Roux CW . Bariatric surgery and hypertension. Surg Obes Relat Dis 2009; 5: 615–620.
Bueter M, Miras AD, Chichger H, Fenske W, Ghatei MA, Bloom SR et al. Alterations of sucrose preference after Roux-en-Y gastric bypass. Physiol Behav 2011; 104: 709–721.
Bueter M, Lowenstein C, Olbers T, Wang M, Cluny NL, Bloom SR et al. Gastric bypass increases energy expenditure in rats. Gastroenterology 2010; 138: 1845–1853.
Le Roux CW, Bueter M, Theis N, Werling M, Ashrafian H, Lowenstein C et al. Gastric bypass reduces fat intake and preference. Am J Physiol Regul Integr Comp Physiol 2011; 301: R1057–R1066.
Le Roux CW, Borg C, Wallis K, Vincent RP, Bueter M, Goodlad R et al. Gut hypertrophy after gastric bypass is associated with increased glucagon-like peptide 2 and intestinal crypt cell proliferation. Ann Surg 2010; 252: 50–56.
Mathes CM, Bueter M, Smith KR, Lutz TA, Le Roux CW, Spector AC . Roux-en-Y gastric bypass in rats increases sucrose taste-related motivated behavior independent of pharmacological GLP-1-receptor modulation. Am J Physiol Regul Integr Comp Physiol 2012; 302: R751–R767.
Chambers AP, Jessen L, Ryan KK, Sisley S, Wilson-Perez HE, Stefater MA et al. Weight-independent changes in blood glucose homeostasis after gastric bypass or vertical sleeve gastrectomy in rats. Gastroenterology 2011; 141: 950–958.
Pezeshki A, Muench GP, Chelikani PK . Short communication: expression of peptide YY, proglucagon, neuropeptide Y receptor Y2, and glucagon-like peptide-1 receptor in bovine peripheral tissues. J Dairy Sci 2012; 95: 5089–5094.
Livak KJ, Schmittgen TD . Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods 2001; 25: 402–408.
Schmittgen TD, Livak KJ . Analyzing real-time PCR data by the comparative C(T) method. Nat Protoc 2008; 3: 1101–1108.
Kisielinski K, Willis S, Prescher A, Klosterhalfen B, Schumpelick V . A simple new method to calculate small intestine absorptive surface in the rat. Clin Exp Med 2002; 2: 131–135.
Cummings BP, Bettaieb A, Graham JL, Kim J, Ma F, Shibata N et al. Bile-acid-mediated decrease in endoplasmic reticulum stress: a potential contributor to the metabolic benefits of ileal interposition surgery in UCD-T2DM rats. Dis Model Mech 2013; 6: 443–456.
Wang TT, Hu SY, Gao HD, Zhang GY, Liu CZ, Feng JB et al. Ileal transposition controls diabetes as well as modified duodenal jejunal bypass with better lipid lowering in a nonobese rat model of type II diabetes by increasing GLP-1. Ann Surg 2008; 247: 968–975.
Cummings BP, Bettaieb A, Graham JL, Stanhope KL, Kowala M, Haj FG et al. Vertical sleeve gastrectomy improves glucose and lipid metabolism and delays diabetes onset in UCD-T2DM rats. Endocrinology 2012; 153: 3620–3632.
Acknowledgements
This work was supported by a Grant-in-Aid from the Heart and Stroke Foundation of Canada, Canada Foundation for Innovation, and the Koopmans Memorial Research Fund to PKC. AR was supported by studentships from the Natural Sciences and Engineering Research Council of Canada and Faculty of Veterinary Medicine. SN was supported by a graduate scholarship from the Faculty of Veterinary Medicine and a Queen Elizabeth II Graduate Scholarship. We appreciate the help of Imran Shah, David Min and Adel Pezeshki.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Author contributions
SN and PKC designed the study, AR and SN performed experiments, AR, SN and PKC conducted the tissue analyses, AR and PKC were responsible for the analysis and interpretation of data, PKC obtained funding, AR drafted the manuscript, AR, SN, PKC undertook the critical revision of the manuscript for important intellectual content and AR, SN and PKC approved the final version of the manuscript.
Supplementary Information accompanies this paper on International Journal of Obesity website
Supplementary information
Rights and permissions
About this article
Cite this article
Ramzy, A., Nausheen, S. & Chelikani, P. Ileal transposition surgery produces ileal length-dependent changes in food intake, body weight, gut hormones and glucose metabolism in rats. Int J Obes 38, 379–387 (2014). https://doi.org/10.1038/ijo.2013.201
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ijo.2013.201
Keywords
This article is cited by
-
Transcriptional and epigenetic changes after dietary and surgical weight loss interventions in an animal model of obesity
International Journal of Obesity (2023)
-
Individuals with type 2 diabetes have higher density of small intestinal neurotensin-expressing cells
Molecular and Cellular Biochemistry (2023)
-
Improvement of Postprandial Lipid Metabolism After Ileal Transposition in Non-obese Diabetic Rats
Obesity Surgery (2021)
-
Biliopancreatic Limb Length of Small Intestinal Bypass in Non-obese Goto-Kakizaki (GK) Rats Correlates with Gastrointestinal Hormones, Adipokines, and Improvement in Type 2 Diabetes
Obesity Surgery (2021)
-
Ileal Transposition in Rats Reduces Energy Intake, Body Weight, and Body Fat Most Efficaciously When Ingesting a High-Protein Diet
Obesity Surgery (2020)
