
Abstract
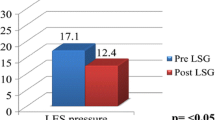
Laparoscopic sleeve gastrectomy (LSG) is effective as a stand-alone bariatric procedure. Despite its positive effect with regard to weight loss and improvement of obesity-related co-morbidities, some patients develop gastroesophageal reflux symptoms postoperatively. The pathogenesis of these symptoms is not completely understood. Hence, this study aimed to assess the effect of sleeve gastrectomy on acid and non-acid gastroesophageal reflux, reflux symptoms and esophageal function. In a prospective study, patients underwent esophageal function tests (high-resolution manometry (HRM) and 24-h pH/impedance metry) before and 3 months after LSG. Preoperative and postoperative symptoms were assessed using the Reflux Disease Questionnaire (RDQ). In total, 20 patients (4 male/16 female, mean age 43 ± 12 years, mean weight 137.3 ± 25 kg, and mean BMI 47.6 ± 6.1 kg/m2) participated in this study. GERD symptoms did not significantly change after sleeve gastrectomy, but other upper gastrointestinal symptoms, particularly belching, epigastric pain and vomiting increased. Esophageal acid exposure significantly increased after sleeve gastrectomy: upright from 5.1 ± 4.4 to 12.6 ± 9.8 % (p = 0.003), supine from 1.4 ± 2.4 to 11 ± 15 % (p = 0.003) and total acid exposure from 4.1 ± 3.5 to 12 ± 10.4 % (p = 0.004). The percentage of normal peristaltic contractions remained unchanged, but the distal contractile integral decreased after LSG from 2,006.0 ± 1,806.3 to 1,537.4 ± 1,671.8 mmHg · cm · s (p = 0.01). The lower esophageal sphincter (LES) pressure decreased from 18.3 ± 9.2 to 11.0 ± 7.0 mmHg (p = 0.02). After LSG, patients have significantly higher esophageal acid exposure, which may well be due to a decrease in LES resting pressure following the procedure.
Similar content being viewed by others

References
Buchwald H, Oien DM. Metabolic/bariatric surgery worldwide 2011. Obes Surg. 2013;23(4):427–36.
Sammour T, Hill AG, Singh P, et al. Laparoscopic sleeve gastrectomy as a single-stage bariatric procedure. Obes Surg. 2010;20(3):271–5.
Deitel M, Gagner M, Erickson AL, et al. Third International Summit: Current status of sleeve gastrectomy. Surg Obes Relat Dis. 2011;7(6):749–59.
Himpens J, Dapri G, Cadiere G. A prospective randomized study between laparoscopic gastric banding and laparoscopic isolated sleeve gastrectomy: results after 1 and 3 years. Obes Surg. 2006;16:1450–6.
Gagner M, Deitel M, Kalberer TL, et al. The Second International Consensus Summit for Sleeve Gastrectomy. Surg Obes Relat Dis. 2009;5(4):476–85.
Rosenthal RJ et al. International Sleeve Gastrectomy Expert Panel Consensus Statement: best practice guidelines based on experience of 12,000 cases. Surg Obes Relat Dis. 2012;8(1):8–19.
Hampel H, Abraham NS, El-Serag HB. Meta-analysis: obesity and the risk for gastroesophageal reflux disease and its complications. Ann Intern Med. 2005;143(3):199–211.
Pandolfino JE, El-Serag HB, Zhang Q, et al. Obesity: a challenge to esophagogastric junction integrity. Gastroenterology. 2006;130(3):639–49.
Chiu S, Birch DW, Shi X, et al. Effect of sleeve gastrectomy on gastroesophageal reflux disease. Surg Obes Relat Dis. 2011;7:510–5.
Mahawar KK, Jennings N, Balupuri S, et al. Sleeve gastrectomy and gastro-oesophageal reflux disease: a complex relationship. Obes Surg. 2013;23:987–91.
Klaus A, Weiss H. Is preoperative manometry in restrictive bariatric procedures necessary? Obes Surg. 2008;18(8):1039–42.
Braghetto I, Lanzarini E, Korn O, et al. Manometric changes of the lower esophageal sphincter after sleeve gastrectomy in obese patients. Obes Surg. 2009 Nov.
Berende CA, de Zoete JP, Smulders JF, et al. Laparoscopic sleeve gastrectomy feasible for bariatric revision surgery. Obes Surg. 2012;22(2):330–4.
Shaw MJ, Talley NJ, Beebe TJ, et al. Initial validation of a diagnostic questionnaire for gastroesophageal reflux disease. Am J Gastroenterol. 2001;96(1):52–7.
Bredenoord AJ, Fox M, Kahrilas PJ, et al. Chicago classification criteria of esophageal motility disorders defined in high resolution esophageal pressure topography. Neurogastroenterol Motil. 2012;24 Suppl 1:57–65.
Khajanchee YS, Cassera MA, Swanström LL, et al. Diagnosis of Type-I hiatal hernia: a comparison of high-resolution manometry and endoscopy. Dis Esophagus. 2013;26(1):1–6.
Soricelli E, Iossa A, Casella G, et al. Sleeve gastrectomy and crural repair in obese patients with gastroesophageal reflux disease and/or hiatal hernia. Surg Obes Relat Dis. 2013;9(3):356–61.
Wu JC, Mui LM, Cheung CM, et al. Obesity is associated with increased transient lower esophageal sphincter relaxation. Gastroenterology. 2007;132(3):883–9.
Melissas J, Koukouraki S, Askoxylakis J, et al. Sleeve gastrectomy: a restrictive procedure? Obes Surg. 2007;17:57–62.
Conflict of interest
Jan. S. Burgerhart, Charlotte A.I. Schotborgh, Erik J. Schoon, Paul C. van de Meeberg, Peter D. Siersema, André J.P.M. Smout have no financial or other conflicts of interest related to this publication. Johannes F. Smulders received an educational grant from Covidien PLC, Dublin, Ireland.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Burgerhart, J.S., Schotborgh, C.A.I., Schoon, E.J. et al. Effect of Sleeve Gastrectomy on Gastroesophageal Reflux. OBES SURG 24, 1436–1441 (2014). https://doi.org/10.1007/s11695-014-1222-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-014-1222-1